5212 Claremont Avenue
Oakland, CA 94618• Mon. • Wed. • Fri. • 10am-6:30pm (by appt.) •
• Tues. 12pm-8pm & Thurs. 9am-4pm (by appt.) •Foot Pain
The architecture of the foot and ankle is exquisitely designed to be a mobile yet stable structure that can flexibly adapt to various walking surfaces, yet turn into a spring at the right moment to propel the body forward.
At heel strike, the foot which has traversed the length of the stride from what is called “toe-off” is ready to transform again to the flexible, adaptable structure…then back again to a spring and so on.
The calcaneus is the technical name for the heel bone. Heel strikes on asphalt and concrete can, over time create problems. Imagine taking a fall on asphalt or concrete — there’s no question one would sustain more injury than in falling on a soft surface. For most of us, the walking we do every day is almost exclusive on very hard surfaces. We could easily argue that these hundreds of daily footfalls are repetitive unnatural encounters, and over time this repetitive stress injury to the feet causes pain and foot dysfunction.
Today, Plantar Fascitis is a popular misdiagnosis.
Many people experience pain in the heel, and are told that it is due to a stiffening of the connective tissue jacketing the muscles of the arch (the plantar fascia). However, 100% of the time I find that the culprit is that the heel bone (calcaneus) is not properly aligned with the ankle bone (talus).
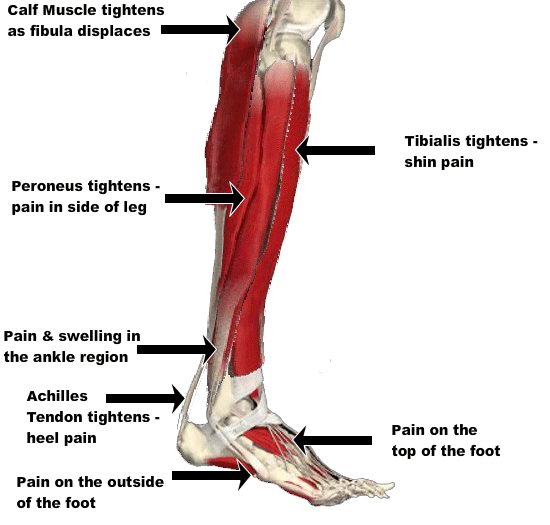
Those are two separate bones; the ankle bone, called the talus, fits up underneath the two knobs that we call the ankle joint, actually the lower tibia and fibula, into what is called a mortise joint (see illustrations). That bone, the talus, the ankle bone, rotates underneath this joint of the lower leg but attached to the underside of it by three joints in three different planes is the heel bone.
This joint complex, the talocalcaneal joint, is the toughest joint in the body. It is resilient, mobile, and amazingly functional when it is healthy. But when the talocalcaneal joint is injured, the continued heel strikes on asphalt and concrete can become a source of great pain and difficulties in walking will result.
The plantar fascia goes from the back of the heel bone all the way across the underside of the foot and into the toes.
It is a very tough, fibrous structure that is part of the mechanism for propelling your body, turning the foot into a spring to propel you forward.

If the heel bone is misaligned in a backward direction (away from the toes), the tissues of the plantar fascia will become over-stretched, irritated and inflamed, to the point of excruciating pain. Restoring the heel bone to its normal position through chiropractic adjustments (back towards the toes) is by far the most efficacious way to deal with this. Proper footwear is also an important part of the recovery from this problem.
Big toe pain shares many of the same features as plantar fascitis. Many big toe pain complaints from patients actually have their origin in a displaced calcaneus.

In these cases, the calcaneus is misaligned in a lateral direction, meaning that it has moved towards the outside (away from the midline of the body). This causes the tendon for the big toe (the hallucis longus), which anchors on the inside of the heel bone, to become over-stretched. This can actually be seen when someone is barefoot and walking away from you; you will see their heel flex away from their midline as they go through the weight-bearing and toe-off phase of their foot on the floor.
This will almost invariably overstretch the tendon, and the pain will be felt where that it crosses underneath the knuckle at the base of the big toe (the metatarsophalangeal joint). Usually digital palpation — putting one’s fingers on it and moving it around when the foot is at rest — does not provoke the pain response that the toe-off motion of the foot does. If I manually hold the heel in its proper position, the entire problem is eased and the toes and their tendons become pain-free. But as soon as I let it go, the problem and the pain comes right back.
Chiropractic adjustment is, again, the only way properly to deal with this condition.
Surgical procedures (such as tendon-scraping and the putting of grooves in metatarsals) are often prescribed by doctors, but prove ineffective because they are not based in a sound anatomical understanding. By restoring the architectural alignment of the foot and ankle, you change the arrangement of all the tendinous structures and remove their distress.
Next, we need to look at how ergonomic considerations can affect leg and foot pain.
This is something that has to be done on an individual basis; many people who have complaints of foot and leg pain also have personal habits that can aggravate an injury. An example of this could be a simple habit like putting one foot and ankle underneath the opposite one when sitting, or tucking one’s right leg underneath the left thigh every time one sits down; normally, when all components are healthy, these habits do not cause pain and are not a direct cause of inflammation or injury. But fall off your bike, bang your right lower leg, and then that life-long habit might be one factor in preventing the right lower leg injury from fully recovering.
So personal habits like how you cross your ankles or your knees or your legs when you are at the computer, the dinner table, sitting on the sofa, or in bed, can be a factor in recovering from a specific injury. These habits need to be carefully analyzed; the patient’s body awareness is a major factor in this pursuit of personal observation. My statement to my patients is that, short of having a camera crew follow you around, I need to have you pay attention to how you manage the lower leg that is injured.
Other habitual uses of the body that can exacerbate an injury include activities like driving. In the case of a right leg injury, continued use of the right foot and ankle to operate the car is not therapeutic. If one has a left leg injury and operates a vehicle with a clutch, this is an issue. These are all considerations that are very, very important in the management of these types of injuries. I find that so many people do not look at the use of their limbs on a daily basis — uses that pre-date the injury, have now become a factor in their continued pain.
Footwear is also very important in an environment of unnatural surfaces.
Heel strike on asphalt and concrete have been shown to cause micro-trauma to the lumbar spine. This stress travels in a kinetic chain, originating in the foot. I recommend supportive footwear that mimics the earth to the foot. Heel strike on earth is absorbed by the earth. Does your footwear transmit the forces back up into your body?
Club Foot is a congenital deformity of the foot. You are born with it, not necessarily inheriting it. You can have it develop in the womb because of deforming forces.
Basically, the kid gets smushed. This happened to my youngest daughter. Her right foot was deformed. The foot was twisted out from underneath the lower leg joint. It would probably have been diagnosed as a “Talipes Valgus” with the heel turned away from the midline. When you looked at her right side of her body you saw the underside of her right foot. The top of her ankle bone was out from underneath the leg and turned sideways. All the attending medical staff in the delivery room said she needed to see a pediatric surgeon.
I started to adjust her the day of her birth. I tried to do it every day, but I know I didn’t. By the time she was 4 ½ months old I could hold her up and she would push against my abdomen. She was loading both feet equally and the foot, though still not appearing quite right, would straighten out with pushing against me. At the age of seven months she was crawling and pulling her self up on to her feet and the right foot was normal in appearance and function.