5212 Claremont Avenue
Oakland, CA 94618• Mon. • Wed. • Fri. • 10am-6:30pm (by appt.) •
• Tues. 12pm-8pm & Thurs. 9am-4pm (by appt.) •Headaches

Headaches can manifest in several ways…
- pain and throbbing at the temples
- pain, pressure and throbbing behind the eyes
- pain or pressure in, behind or over the ears
- muffled hearing
- pressure and throbbing in the sinus cavity
- tightening of the scalp or neck
Headaches can have many sources…
One very common source of headaches is the sternocleidomastoid muscle (SCM), which arises off the sternum and the clavicle and has a large tendon attached to each, one on each side of the joint. The two tendons turn into a strap-like muscle that goes up to the base of the skull, the mastoid process, hence the name “sternocleidomastoid” muscle.
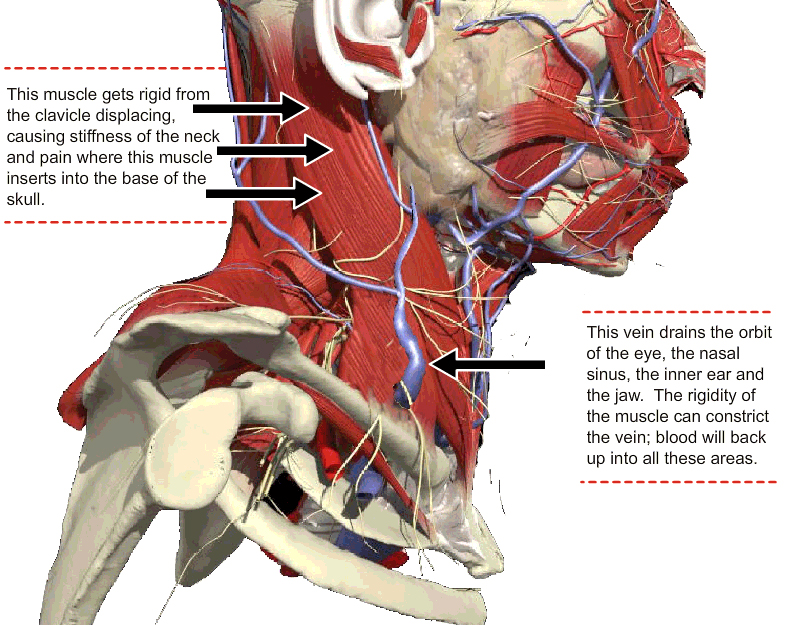
The Sternocleidomastoid Muscle (SCM)
The mastoid process is the big knobby bone at the base of the skull, underneath and behind the ear. The SCM attaches to the two bones in the top of chest and then sweeps up like a fan underneath the ear to the side of the skull. If the clavicle starts to separate from the sternum, the SCM will become rigid to keep it stable. Pain can then develop behind the ear and up the whole side of the head.
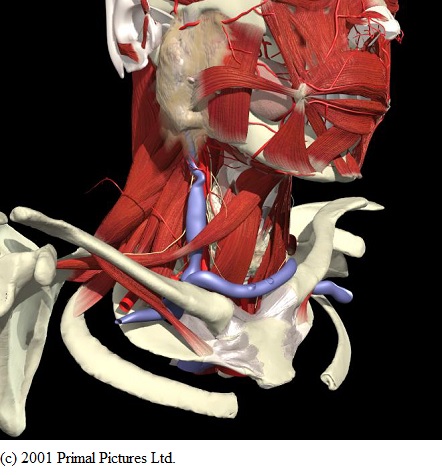
The Sternoclavicular Joint
When injured and subluxated (misaligned), it can also interfere with swallowing. The muscles that attach to the thyroid cartilage and the underside of the hyoid bone go to the inside and posterior back surface of the Sternoclavicular joint. These joints coming apart can actually make the throat muscles tighter than normal, interfering with their function in swallowing.
The Throat Muscles
A tightening of the SCM muscle will limit the range of motion of the head and neck. But this rigidity can have other consequences, because the SCM has in it the External Jugular Vein. The External Jugular Vein drains the “superficial structures” of the head and face; that is, the orbit of the eye, the nasal sinus, the inner ear and the scalp.
The External Jugular Vein
If this vein is compressed by a spasm of the SCM, there can be the sensation of throbbing and increased pressure in any or all of the areas drained by the External Jugular Vein. When the vein backs up and fills, it will be felt as throbbing or pressure behind the eye.This can also happen to the nasal sinus. When the veins of the nasal sinus become engorged, not only will they become clogged and not allow normal passage of air, but they can also start to drip because of their abnormal state of engorgement with fluid. The nasal sinus will start to drip onto the top of the soft palate over the roof of the mouth. This fluid will roll off the back edge of the soft palate onto the epiglottis, which is the top of the throat, resulting in a dry, unproductive and, in many cases, persistent cough.
In addition to the orbit of the eye and the nasal cavity, the External Jugular Vein drains the inner ear. If the vein is compressed within a rigid SCM, the area of the inner ear will become filled and results are muffled or reduced hearing and possibly some vertigo or balance problems. On inspection of the ear it will appear that there is fluid within the inner ear. Often it is assumed that there is an infection, and an antibiotic is prescribed. I believe it is inappropriate – not to mention irresponsible – to prescribe antibiotics without taking a culture and identifying a specific organism. Indiscriminate use of antibiotics has led to the development of resistant strains of bacteria.
Tension headaches are sometimes caused by the SCM itself. The muscle attaches across the side of the head (see illustrations), where the Sharpey’s Fibers insert into the skull.
The Sharpey’s Fibers can become inflamed and irritated when the area is thrown into a guarding response, exerting a constant tension to hold the clavicle to the sternum. The vascular network of arterioles (the small arteries) and capillaries (microscopic blood vessels), can also become compromised with this constant tension (see About Pain section). The resultant reduced blood flow reduces the amount of oxygen supplied to the muscular tissues along the side of the head and scalp, which can produce a pain pattern in itself. Lack of oxygen, called hypoxia, has been known to be a painful condition causing burning and aching sensations.
So, all of the headache symptoms above can be set off by an injury to the top of the chest, the Sternoclavicular joint. This can be caused by commonplace events such as:
- a seat belt straining across the clavicle
- a fall
- yanking on something that will not move, like a door that is stuck
- rough-housing with a three year-old
- being pulled off balance by a dog
Such an event can result, even weeks or months later, in constant, persistent head pain. These are all common events. Few people ever look to the top of the chest as a source of pain for the head
Upper Cervical Vertebra and Suboccipital Muscles
Finally, the misalignment (subluxation) of the upper cervical spine is another common source of headaches. Quite a few of the muscular structures that attach to the vertebrae also attach to the head. The same phenomenon we discussed above, of muscles attached at one joint causing pain at another part of the body, can occur here. In this case the suboccipital muscles, which attach at one end to the vertebrae, can become very painful at their other end where they attach to the base of the skull.
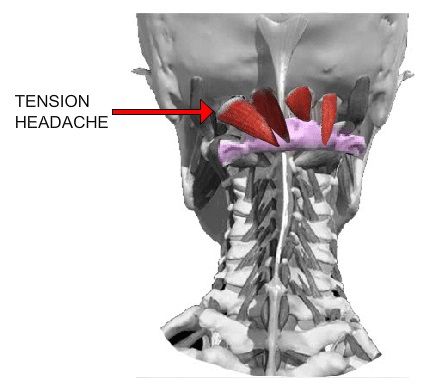
When a misalignment or subluxation pattern of the upper cervical vertebrae take place, the suboccipital muscles will reflexively tighten to protect the vital structures of the region. This rigidity can also be a source of pain in itself and can again compromise the arteriole structures and venous structures. Muscular guarding, which is the body’s attempt to hold everything inflexibly in order to keep it from going any further out of place, is an appropriate defensive response but can cause constant, unrelenting pain, not relieved by either rest or medications.