5212 Claremont Avenue
Oakland, CA 94618• Mon. • Wed. • Fri. • 10am-6:30pm (by appt.) •
• Tues. 12pm-8pm & Thurs. 9am-4pm (by appt.) •Knee Pain
Knee pain is common, and where the knee hurts is an important aspect of diagnosing the problem.
Some people have the pain in the area below the knee cap; others, to one side of the knee cap, or behind the knee, or to the inside or outside of the knee.
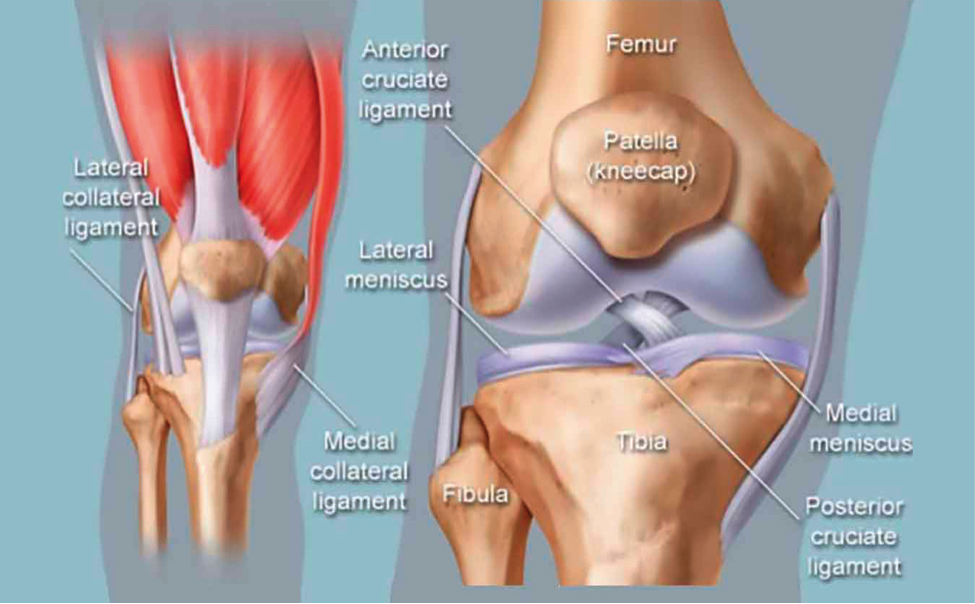
The causes are usually “mechanical” in nature (although I prefer the term “architectural”). The knee is a joint between the femur (the long, thick thigh bone) and the tibia (the larger of the pair of bones in the lower leg between the ankle and the knee). When the tibia is not properly aligned with the femur, the joint doesn’t work quite right and pain and limited motion can be the result. (See Figure 1)
How the knee is misaligned, or which direction the tibia is displaced, has a large influence on where it hurts.
In my research of the definitions and explanations of knee arthritis, it is always described as “having no known cause.” Yet in 22 years, I have never encountered a case of arthritis of the knee in which the tibia was properly aligned with the femur.
The knee joint is designed, when properly aligned, to bear the upper body’s weight and to move, pain-free, through its normal range of motion. When the alignment is altered, the knee ligaments and meniscus are stressed, causing degenerative change – otherwise known as arthritis.
The cause of knee arthritis is the persistent displacement (subluxation) of the tibia and femur. Trauma to the knee is the most common source of knee misalignment, and therefore knee pain.
Because orthopedic medicine simply does not recognize the existence of this condition, the typical orthopedic patient will never get his/her knee bones restored to their proper alignment as a part of treatment.
Thus, while the patient is told to “take your pills and exercise”, the knee joint is actually being allowed to degenerate. Any misalignment of the two bones will injure the meniscus (a disk of cartilage that serves as a cushion between the ends of bones that meet at a joint) and cruciate ligaments.
Sometimes surgery is required to repair the damaged ligaments and/or meniscus. These repairs can be very helpful, but wouldn’t proper alignment of the bones as well result in the very best outcome? Yet most knee surgery patients never have their joints realigned.
Postural distortion is another way to injure the knee. Too much sitting, kneeling or other persistent deforming of the knee can leave the bones misaligned.
This is particularly true if there is a history of falling on bent knees (like Pete Townshend doing a rock and roll slide, or a break-dancer), or if one’s job requires kneeling– tile-setting or floor work, for instance.
The patterns of displacement can be complex, so each knee needs to be individually examined and evaluated.
Sideways forces are common, displacing the bones towards the inside or the outside, and the knee is subject to twisting forces as well. I have patients with different subluxation patterns in each knee; I tell them they’re lucky they only have two, otherwise things could get complicated!
My own knees have been injured in external rotation with a lateral (outside) shift and hyperextension (backwards). I keep my knees active and they get adjusted at least once, if not twice a week. They are minimally sore and rarely stop me from doing what I want to do.
In our office we do gentle adjusting, as opposed to manipulation of the knee. I prefer this approach to my own knee problems and I find most patients do as well.